
Medicine itself is sick – you’ve probably heard it many times.
And you likely know why: on average, 97% of healthcare spending goes to treatment and 3% to prevention; care is fragmented, and doctors are overburdened with administrative work. We hardly understand any disease and, therefore, need to treat symptoms chronically but not the causes.
But the list of errors in today’s medicine is much longer.
In the book “The end of medicine as we know it – and why your health has a future”, Prof. Harald H. H. W. Schmidt uncovers them all. I met Prof. Schmidt to find out what the way out of sick medicine is.

Before reading the interview, a summary of the book.
Prof. Schmidt explains 9 pathologies (plagues) in healthcare:
- The organ-centric view of medicine has led to an impasse.
- Prevention is neglected.
- Since diseases can neither be prevented nor cured, many become chronic.
- Life expectancy is stagnating and, in some countries, declining.
- Men, and people with lower socio-economic status, live shorter.
- Biomedical research is highly irreproducible, of poor quality, and not patient-focused.
- Healthcare providers are given false incentives to commercialize against patient welfare.
- Very few patients benefit from their medicines and therapies.
- Big Pharma is not sustainable in its current form.
The second part (Medicine of The Future) reveals what must be done to end the crisis:
- Medicine must start thinking and acting systematically. Quality, not quantity, must become the essential incentive.
- Pharma companies must be judged whether their therapies cure rather than treat symptoms chronically.
- Biomedical scientists must have patient well-being as their goal, not a perverted pursuit of printed paper in high-impact journals.
- Biomedical research and health policies must focus on improving health literacy and removing social gaps in healthcare.
- And you should demand – and accelerate – a transformation in healthcare by using breakthrough technologies like symptom checkers wearables.
So we have to fix the broken system, right?

Artur Olesch: Health systems are based on false incentives; research is made for the sake of being published, and medicine is organ-based. We are being prescribed medicines that do not always work while doctors treat the symptoms instead of being a source of chronic diseases. What’s even worse, the socio-economic gaps in healthcare are rising. Still, in high-income countries, patients seem to be ok with that. So, is healthcare really in crisis?
Harald Schmidt: To be unhappy, one must know that a happier state is possible.
The current age group of patients 60+ stems from a generation that blindly trusts what a doctor diagnosed and suggested. They almost leave the entire responsibility of their health in the hands of their doctor.
My book aims to provide the facts that “eating what is served” is not always the best choice.
In the USA, the UK and some European countries, life expectancy has recently declined while costs still go up. With the diabetes pandemic, prospects are grim. The sharpest weapon against disease (i.e., prevention) is essentially unused. Drug therapy or a quick fix is preferred by doctors, and patients are highly inefficient.
Antihypertensives are my favorite example – they lower blood pressure for most patients. But that’s not the goal. We prescribe antihypertensives to prevent a stroke or heart attack, and it needs 100 patients to be treated to prevent one of these events. Patients are unaware of this, but what shocks me quite frequently is that even doctors are.
They think they benefit every patient for whom they prescribe such a drug or drug cocktail.
Another area is orthopedic surgery – one of the biggest income streams for most hospitals. Numerous studies have shown that knee arthroscopy, shoulder, back, and hip surgeries provide no benefit for most patients or none above placebo surgery. We have a sick-care system where input is reimbursed, but no one measures output or patient value.
It’s the latter that should be reimbursed.
The “disease healthcare system” – as you call it – has been created for decades. It could be better, sure. But could we have done it better without all the new technologies and know-how we have now?
All our current technologies have provided minimal benefit. The most important reason for the rise in life expectancy since 1900 is a reduction in newborn deaths and the prevention and treatment of infections: hygiene, vaccinations, and antibiotics.
We could have done better by reimbursing only validated patient benefits and focusing much more on prevention. Unfortunately, the latter is an area that goes beyond medical training and requires a team approach with many other healthcare providers.
To end this crisis, you suggest leveraging genomics, Big Data, and technologies like wearables or apps. For this to succeed, we need a system shift and to start using all the innovations.
Yes, first, we need a completely new definition of “disease”.
Currently, we use 21st-century technology on 19th-century disease definitions. Sequencing the human genome has achieved nothing for most diseases. Hypertension, asthma, ulcerous colitis, heart failure, chronic kidney disease, psoriasis, etc., are just descriptive umbrella terms of organ symptoms.
There is no actionable understanding of the molecular causes available.
Thus, doctors only have the option of treating symptoms with very low effectiveness. Most likely, each symptom has several different causes, each needing another curative therapy. Therefore, we need to restructure medicine completely (i.e., give up the organ-based structure where we have a clinic, a specialist, and a research discipline for every organ).
Instead, we need to unite all disciplines and symptoms to discover the underlying mechanisms, irrespective of which organ they occur. Rare diseases are already at this level. Each is caused by a single gene and is, thus, precisely named after that gene. Diagnosis and therapy are crystal clear. Over the next decade, they will all be curable by gene editing.
Most other diseases are caused by several genes plus lifestyle, and we have made zero progress here.

You admit that we still don’t know enough about how our bodies – extremely complex ecosystems – work. How can we personalize prevention if there are still so many open questions? A lot can go wrong.
In the same way that we will redefine diseases and make therapy precise and curative, we will also improve prevention.
Prevention currently has the issue that everything is suggested to everyone: don’t smoke, go low on alcohol, sleep well, exercise, eat little meat and sugar, use early cancer detection offerings, etc. Not wrong, but unachievable for most. Precision prevention will focus on one or two key lifestyle measures for which there is a molecular reason and monitor the success and sufficiency.
The future healthcare you envision sounds appealing – at least from medicine’s perspective. But isn’t it wishful thinking that Big Pharma suddenly invest in prevention and people will change their habits and start listening to a fridge saying that another bottle of wine is not a good idea? It sounds like turning business models and our lives upside down.
Yes, that’s what many futurologists predict.
It will be the next Kondratieff wave. These come every 40 years and make established industries and concepts disappear while new ones appear.
Think of the recent IT revolution and what it has changed. Similar ones were due to automobiles, electricity, or the steam engine. Big Pharma has been in a constant efficacy decline since the 1950s – we will soon have all the drugs that we need. We only need to apply them precisely for the right patient.
And patient empowerment will be a necessity. For example, everyone takes their car for an inspection and thoroughly studies flat-screen TV specs before buying one. So, why should people not take more control over their most precious asset – their body?
Lower education and social status now cost you eight years of healthy life expectancy.
There are three perspectives in the discussion about future medicine that must be considered: human nature (and needs), science, and ethics. Do we already have to think about the right to “not to know” about possible health risks, broken genes, or diseases that still don’t show symptoms?
In Europe, this would be no issue.
Health insurance companies would probably offer incentives. In the USA, I’m more skeptical because health insurers currently exclude pre-existing conditions, charge exorbitant premiums, or even reject patients. The USA lacks a societal solidaristic system ensuring that no one runs the risk of personal bankruptcy just because of an illness.
What tech innovation has immense potential to speed up this revolution?
Scientifically, it’s less complicated than one might think.
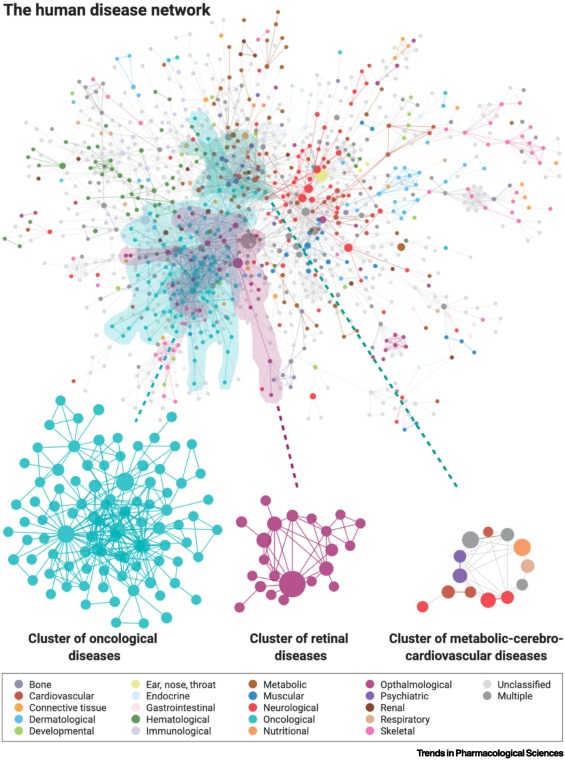
The only step we need to do is correctly interpret all the genetic information we already have from millions of patients to discover hidden underlying causal mechanisms in these patterns. This field already exists and is called “systems or network medicine”.
In fact, we and others are already running several high-precision clinical trials that will provide data in 2023. When they are positive, I predict an avalanche of change for the whole of medicine. The minimum technology you need as a patient is to have your genome sequenced, which on Black Friday costs (approximately) no more than $200.
If you then want to have – on top of that – an objective (!) overview of your lifestyle without betraying yourself, an electronic health record such as Apple Health would help. That’s about it. You have generated a digital twin of yourself that can tap into the wealth of knowledge explosion the new medicine will offer you.
And the last question: what are three takeaways from your book “The end of medicine we know it – and why your health has a future” for doctors, politicians, and all of us?
Doctors and hospitals need to become humbler, less profit-oriented, and start working in interdisciplinary teams that provide prevention so that a patient never needs to see a doctor.
Politicians need to understand the status of medicine and induce the necessary changes in research and practice top-down. It is nothing but a paradigm shift.
Thank you for your time!
P.S. The end of medicine as we know it – and why your health has a future‘ (available on Amazon) describes how medicine has reached the peak of its capabilities within the current (broken) health system framework. This is a well-written book based on solid academic knowledge. However, at times I missed the detachment from the reality of a health system that cannot simply be changed overnight.

Can I ask you a favour?
Please donate to aboutDigitalHealth.com (€1+) and support independent journalism. It only takes a minute. Thank you!
€1.00
